Being able to review a fresh urine sediment can provide you with lots of pertinent information when it comes to renal-urinary tract pathology. It's best to use a fresh sample i.e. reviewed preferrable within minutes of collection.
The sediment depicted in the question displays the flat, square plates, which are characteristic of one form of uric acid crystals. Hyperuricemia may accompany rapid cell turnover which is a potential complication secondary to the rapid lysis of lymphoma cells after chemotherapy. It is important to provide aggressive hydration, give allopurinol and alkalinize the urine to provide effective prophylaxis against uric acid nephropathy.
There are many things you can see in analyzing the urinary sediment. This includes blood:
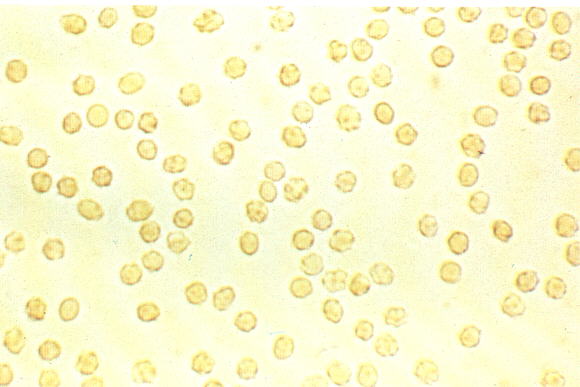
Which if coming from the glomerulus may produce the following dysmorphic RBC's:

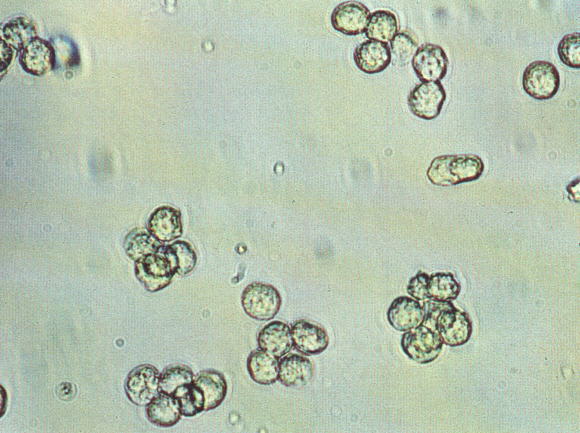
You may also see urine leukocytes:
Associated with leukocytes would be the presence of bacteria. Recall that this is not a gram stain and thus the bacteria do not look the same as they would in the microbiology lab sample:

You may also look for contaminants such as a) squamous cells, b) cotton fibers and c) starch granules respectively:
a)
b)
c) 
You also want to look for particular forms of casts.
The RBC cast of glomerular pathology:

The WBC cast of pyelonephritis:

The nonspecific granular, waxy and hyaline casts:



In contrast many would consider the finding of Broad casts as a sign of the markedly decreased output of chronic renal failure. They are usually quite wide and are upto 2-6 times as wide as the above nonspecific casts (thus the name "broad"):

The pathologic crystals of metabolic diseases and poisonings can be seen as well:
CYSTINE:

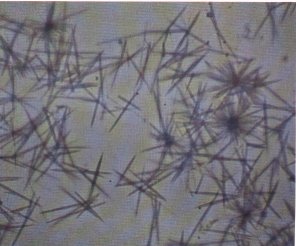
TYROSINE:
CALCIUM OXALATE:

Finally one might find the "coffin-lid" struvite crystals associated with urea-splitting bacteria:

Finally, in patients with nephrotic syndrome one might be able to find fat casts:

References:
![]()