
Urea 25-30
Uric acid 0.6-0.7
Creatinine 1.0-1.2
Hippuric acid 0.7
Ammonia 0.7
Amino acids 3
Sodium 1-5 (NaCl 15.0)
Potassium 2-4
Calcium 0.2-0.3
Magnesium 0.1
Chloride 7
Phosphate 1.7-2.5
Sulfate 1.8-2.5
Routine urinalysis is composed of two examinations:
1) Chemical tests for abnormal chemical constituents
2) Microscopic exam for abnormal insoluble constituents
|
CHEMICAL The common chemical testing of urine utilizes commercial disposable test strips. Bayer's Multistix 10 SG test strips test for Glucose, Bilirubin, Ketone, Specific Gravity, Blood, pH, Protein, Urobilinogen, Nitrite, and Leukocyte Esterase. The result of this testing is regarded as semiquantitative. A fresh urine specimen is collected in a clean, dry container. A Multistix strip is briefly immersed in the urine specimen, covering all reagent areas. The edge of the Multistix strip is run against the rim of the urine container to remove excess urine. The strip is held in a horizontal position. The reactions are read visually or automatically with a Clinitek reflection photometer. If the strip is evaluated visually, the strip test areas are compared to those on the Multistix color chart at the specified times. The results are recorded, and the strip is discarded. |



|
|
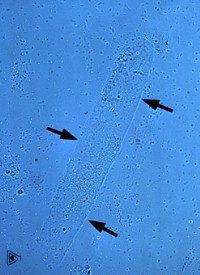
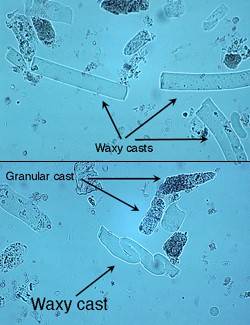
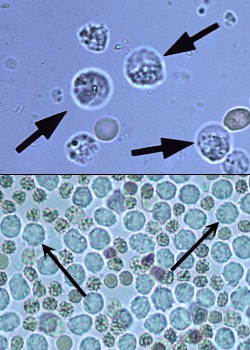
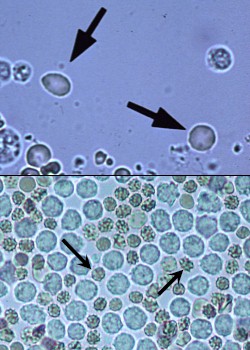
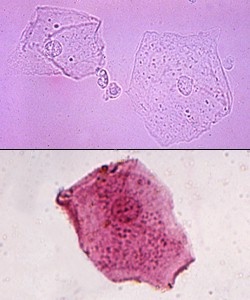
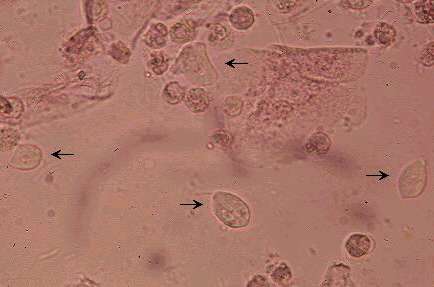
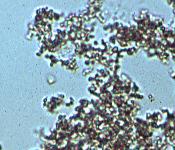
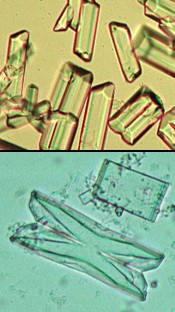
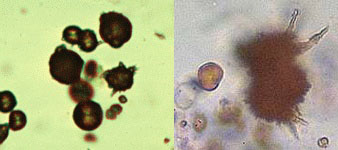
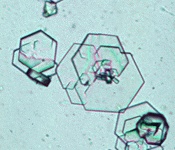
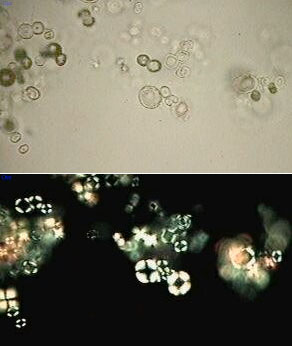
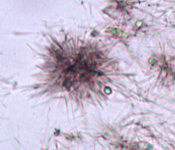
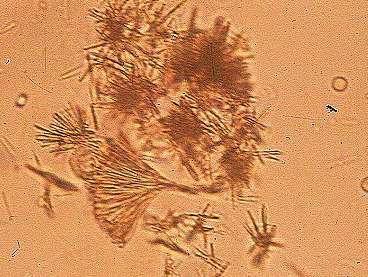
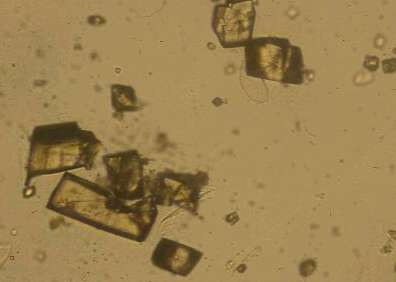
Hyaline casts are formed in the absence of cells in the renal tubular lumen. They have a smooth texture and a refractive index very close to that of the surrounding fluid. When present in lower numbers (0-1/LPF) in concentrated urine of otherwise normal patients, hyaline casts are not always indicative of clinically significant disease. Greater numbers of hyaline casts may be seen associated with proteinuria of renal (eg., glomerular disease) or extra-renal (eg., overflow proteinuria as in myeloma) origin. Click here for a diagram of cast formation. Cellular casts most commonly result when disease processes such as ischemia, infarction or nephrotoxicity cause degeneration and necrosis of tubular epithelial cells. A common scenario is the patient with decreased renal perfusion and oliguria secondary to severe dehydration. Ischemic injury results in degeneration and sloughing of the epithelial cells. The resulting casts often are prominent in urine produced following rehydration with fluid therapy. The restoration of urine flow flushes numerous casts out of the tubules. Leukocytes can also be incorporated into casts in cases of tubulo-interstitial inflammation (eg., pyelonephritis). Budding yeast cells and mucous filaments are also present in the photomicrograph at right. Granular casts have a textured appearance which ranges from fine to coarse. Since they usually form as a stage in the degeneration of cellular casts, the interpretation is similar to that for cellular casts. Sperm cells are also present in the photomicrograph at right. Fatty casts are identified by the presence of refractile lipid droplets. The background matrix of the cast may be hyaline or granular. Often, they are seen in urines in which free lipid droplets are present as well. Interpretation of the significance of fatty casts should be based on the character of the cast matrix, rather than on the lipid content. Pictured is a fatty cast with a hyaline matrix. As an isolated finding, lipiduria is seldom of clinical significance. Waxy casts have a smooth consistency but are more refractile and therefore easier to see compared to hyaline casts. They commonly have squared off ends, as if brittle and easily broken. Waxy casts are found especially in chronic renal diseases, and are associated with chronic renal failure; they occur in diabetic nephropathy, malignant hypertension and glomerulonephritis. Oval Fat Bodies (OFB) are similar in composition and significance to fatty casts. Desmorphic red cells (pictured ar right) are observed in glomerulonephritis. "Dysmorphic" red cells refer to heterogeneous sizes, hypochromia, distorted irregular outlines and frequently small blobs extruding from the cell membrane. White Blood Cells (WBC) in unstained urine sediments typically appear as round, granular cells which are 1.5-2.0 times the diameter of RBCs. WBC in urine are most commly neutrophils. Like erythrocytes, WBC may lyse in very dilute or highly alkaline urine; WBC cytoplasmic granules released into the urine often resemble cocci bacteria. WBC up to 5/HPF are commonly accepted as normal. Greater numbers (pyuria) generally indicate the presence of an inflammatory process somewhere along the course of the urinary tract (or urogenital tract in voided specimens). Pyuria often is caused by urinary tract infections, and often significant bacteria can be seen on sediment preps, indicating a need for bacterial culture. Fresh RBC tend to have a red or yellow color (lower panel). Prolonged exposure results in a pale or colorless appearance as hemoglobin may be lost from the cells (upper panel). In fresh specimens with a Specific Gravity (SG) of 1.010-1.020, RBC may retain the normal disc shape (upper panel). In more concentrated urines (SG>1.025), RBC tend to shrink and appear as small, crenated cells (lower panel). In more dilute specimens, they tend to swell. At a SG<1.008 and/or highly alkaline pH, RBC lysis is likely. Lysed RBC appear as very faint "ghost cells". Red blood cells up to 5/HPF are commonly accepted as normal. Increased RBC in urine is termed hematuria, which can be due to hemorrhage, inflammation, necrosis, trauma or neoplasia somewhere along the urinary tract (or urogenital tract in voided specimens). Squamous epithelial cells are the largest cells seen in normal urine specimens. They are thin, flat cells, usually with an angular or irregular outline and a small round nucleus. They may be present as single cells or as variably-sized clusters. Those shown in the upper panel are unstained; that in the lower panel was prepared using Sedi-Stain. Squamous cells are common in lower numbers in voided specimens and generally represent contamination from the genital tract. Their main significance is as an indicator of such contamination. Parabasal squamous epithelial cells are immature squamous epithelial cells. They are commonly seen in urine specimens from postmenopausal women with atrophic vaginitis resulting from decreased estrogen (estradiol) levels. Transitional epithelial cells originate from the renal pelvis, ureters, bladder and/or urethra. Their size and shape depends on the depth of origin in the epithelial mucosa. Most often they are round or polygonal; less commonly pear-shaped, caudate or spindle-shaped. They are generally somewhat smaller and smoother in outline than squamous cells, but larger than WBC. They may develop refractile, fatty inclusions as they degenerate in older specimens (upper panel). In cleanly-collected normal specimens, transitional cells are few (ca. <2/HPF), but are more frequent in the elderly population. However, the presence of transitional sheets ("brick wall" appearance) is sometimes associated with Transitional Cell Cancer (TCC). Renal Tubular Cells (RTC) are originally cubic in shape; but once exfoliated, they adopt a rounded shape. These cells are slightly larger than leukocytes (10-14 um) with lightly granular cytoplasm. The nucleus is round, well defined and usually centric. The cytoplasm often shows a perinuclear halo when stained. Note the "glitter" cell (fatty degenerated WBC) in the lower-left corner. Trichomonas vaginalis is a sexually-transmitted urogenital parasite of men and women. The organism varies in size between 1-2 times the diameter of WBC. The organism is readily identified by its rapid erratic "jerky" movement. Calcium Oxalate Dihydrate crystals typically are seen as colorless squares whose corners are connected by intersecting lines (resembling an envelope). They can occur in urine of any pH. The crystals vary in size from quite large to very small. Dietary asparagus and ethylene glycol intoxication are notorious for urinary calcium oxalate formation. Calcium Oxalate Monohydrate crystals vary in size and may have a spindle, oval, or dumbbell shape. Most commonly, they appear as flat, elongated, six-sided "fence picket" crystals as seen at the right. Sometimes they closely resemble colorless RBCs. Amorphous crystals appear as aggregates of finely granular material without any defining shape. Amorphous urates of Na, K, Mg or Ca tend to form in acidic urine and may have a yellow or yellow-brown color. Amorphous phosphates are similar in general appearance, but tend to form in alkaline urine and lack color. Generally, no specific clinical interpretation can be made for the presence of amorphous crystals. Triple phosphate (Struvite, Magnesium Ammonium Phosphate) crystals usually appear as colorless, prism-like "coffin lids". They are often seen in urine from clinically normal individuals. Although they can be found in urine of any pH, their formation is favored in neutral to alkaline urine. Urinary tract infection with urease producing bacteria (eg. Proteus vulgaris) can promote struvite crystalluria (and urolithiasis) by raising urine pH and increasing free ammonia. Uric acid crystals may appear as yellow to brown rhombic or hexagonal plates, needles or rosettes. With rare exceptions, the finding of uric acid crystals in urine is of little clinical value. Ammonium urate (or biurate) crystals generally appear as yellow-brown, radially-striated spheres with irregular "thorn-apple" or "ox-horn" projections. Although they may be seen in acid urine, their formation is favored in neutral to alkaline urine. Cystine crystals are seen as flat colorless hexagonal plates. They often aggregate in layers, and their formation is favored in acidic urine. Cystine crystalluria or urolithiasis is an indication of cystinuria, which is an inborn error of metabolism involving defective renal tubular reabsorption of certain amino acids including cystine. Leucine crystals are seen as yellow spheres with concentric and radial strias. These crystals can sometimes be mistaken for cells, with the center resembling a nucleus. Under polarized light, leucine crystals transmit a "maltese cross" interference pattern. Crystals of the amino acids leucine and tyrosine are very rarely seen in urine sediments. These crystals can be observed in some hereditary diseases like tyrosinosis and "Maple Syrup Disease". More often one finds these crystals concurrently in patients with severe (often terminal) liver disease. Tyrosine crystals are usually seen as fine brownish needles, either isolated or as rosettes. These are sometimes associated with severe liver disease. Cholesterol crystalizes as thin rectangular plates with one (sometimes two) of the corners having a square notch. The cause of the presence of crystalized cholesterol is obscure. These crystals are seen in degenerative renal disease and are thought to have an identical clinical meaning as OFB. The presence of cholesterol crystals is usually accompanied by proteinuria, but they are only rarely seen. Sulfadiazine crystals are a common finding with administration of Trimethoprim-sulfadiazine. They are often seen as "shocks of wheat" or radially-striated spherules. Sulfonamide crystals are typically yellow in color and often resemble uric acid crystals. However, sulfa crystals are easily distinguished from uric acid by confirmatory tests. Sulfa crystals are readily soluble in acetone and exhibit a positive dextrine/sulfuric acid test ("old yellow newspaper" test). Many drugs excreted in the urine have the potential to form crystals. Hence, a review of the patient's drug history is useful when an unidentified crystal is found. |
                       |
Test Reference Range
Color Straw - Dark yellow
Appearance Clear - Hazy
Specific Gravity 1.003-1.029
pH 4.5-7.8
Protein Negative
Glucose Negative
Ketones Negative
Bilirubin Negative
Occult blood Negative
Leukocyte Esterase Negative
Nitrite Negative
Urobilinogen 0.1-1.0 EU/dL
WBCs 0-4/hpf
RBCs male: 0-3/hpf
female: 0-5/hpf
Casts 0-4/lpf
Bacteria Negative
EU = Ehrlich Units (ca. 1 mg) hpf = High Power Field (400x) lpf = Low Power Field (100X)
OTHER TESTS
|
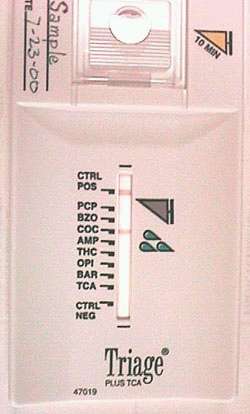
Biosite Diagnostics manufactures a convenient test pack with the proprietary label Triage, which employs a simultaneous competative binding immunoassay for 8 drugs of abuse and their metabolites.
Triage Plus TCA provides a rapid qualitative urine screen that analyzes a single urine sample for the following drugs of abuse: Amphetamines/ Methamphetamines, Cocaine, Opiates (heroin), Phencyclidine (PCP) and Tetrahydrocannabinol (marijuana). Prescription drugs tested: Barbiturates, Benzodiazepines, Tricyclic Antidepressants. As stated above, the method utilizes a competative binding immunoassay in which a chemically labeled drug (drug conjugate) competes with drug which may be present in the urine for monoclonal antibody binding sites. After a brief (10 minutes) incubation of urine with the drug monoclonal antibodies and competing drugs conjugated to colloidal gold, the reaction mixture is transferred to a detection membrane on which are immobilized zones of monoclonal antibodies. Free drug conjugate that is displaced from antibody binding sites by drug in the urine, binds to a zone on the membrane. The membrane is washed to remove the unbound conjugate. Test results are read visually. The photo demonstrates a positive test for cocaine. Positive results |
|
Threshold Detection and Clearance Times of Several Drugs
Drug Cut-off Approximate Detection Time in Urine using EMIT **
Conc.
Amphetamines 1000 ng/mL * 2-4 days
Barbiturates 300 ng/mL * Short-Acting (eg. secobarbital) 1 day.
300 ng/mL * Long-Acting (eg. phenobarbital) 2-3 weeks.
Benzodiazepines 300 ng/mL 3-7 days
Cannabinoids 50 ng/mL 3-30 days (half-life = 7 days)
Cocaine 300 ng/mL * 2-4 days
Codeine ---------- 2-5 days
Euphorics (LSD, XTC) ---------- ? days (Currently, not detectable by EMIT.
Detectable by GC/MS, however)
Methadone ---------- 3-5 days
Methaqualone ---------- 14 days
Opiates 300 ng/mL 2-4 days
Phencyclidine (PCP) 25 ng/mL * 8-14 days
Phenobarbital 300 ng/mL * 10-20 days
Propoxyphene ---------- 6 hours to 2 days
* Recommended SAMHSA cut-off concentrations
** EMIT: Syva Corp. acronym for Enzyme Multiplied Immunoassay Technique
|
|
|
| Search THIS ENTIRE WEB SITE for CLS technical, financial or other data >>> |
 E-mail
Irving E-mail
Irving |
This page is made entirely from recycled electrons. Any similarity between this and any other page may be completely intentional. Not tested on animals. Void where prohibited. Return to Irving's Home Page |